
The below ECG is from a 69 year old male who presented to ED with general malaise and fatigue. The patient is has a background of metastatic colon cancer and depression.
- Describe and interpret the ECG
- The VBG machine is not working, and you need to wait for formal blood results. Choose 2 drugs you would consider using while awaiting investigations results, including dose and route of administration and what on history would make you consider those drugs.
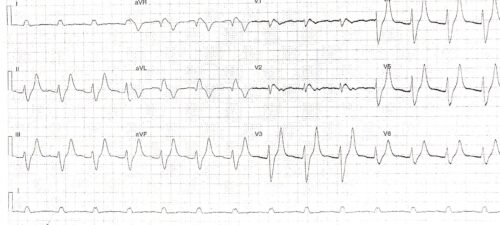
Rate: 84 beats per minute
Rhythm: Sinus rhythm – P waves seen in inferior leads
Axis: Left Axis
Intervals
- PR 200ms
- QRS 160 -200ms
- QT 497ms (Bazett)
Additional:
Really wide QRS. Sine wave pattern V1 aVR
Atypical LBBB pattern
Tall symmetrically peaked T waves
Flattening of P waves
Wide complex sinus rhythm, with tented T waves and border line prolonged PR interval
A rhythm with marked widening of the QRS is associated with
- BBB
- Hyperkalaemia
- Na Channel blockade secondary to toxicological causes
- Preexcitation (WPW)
- Ventricular paced beats
- PVC
In this clinical setting concern about toxicological causes, as patient has a background of depression, and renal failure with hyperkalaemia need to be considered.
On history you would need to look for possible causes of renal failure – bowel obstruction, vomiting, past history of CRF, use of renal toxic medication, as well as history of overdose and prescribed Na channel blocking antidepressants. Other toxicological causes at this HR would be B blockers.
The 2 drugs of choice in this situation when your differential would be hyperkalaemia and Na channel toxicity would be :
- Calcium gluconate 10ml 10% over 10 minutes – repeated to 30ml IV
- NaHCO3 1mmol/kg IV
Both drugs would stabilise the heart in hyperkalaemia and Na channel toxicity. NaHCO3 would also lower the potassium in a patient with acidosis and hyperkalaemia. The drugs can be administered while obtaining further history and awaiting blood results. The changes in the ECG often occur in real time while administering the medication.