
Interpretation of ECG from 16 November 2022
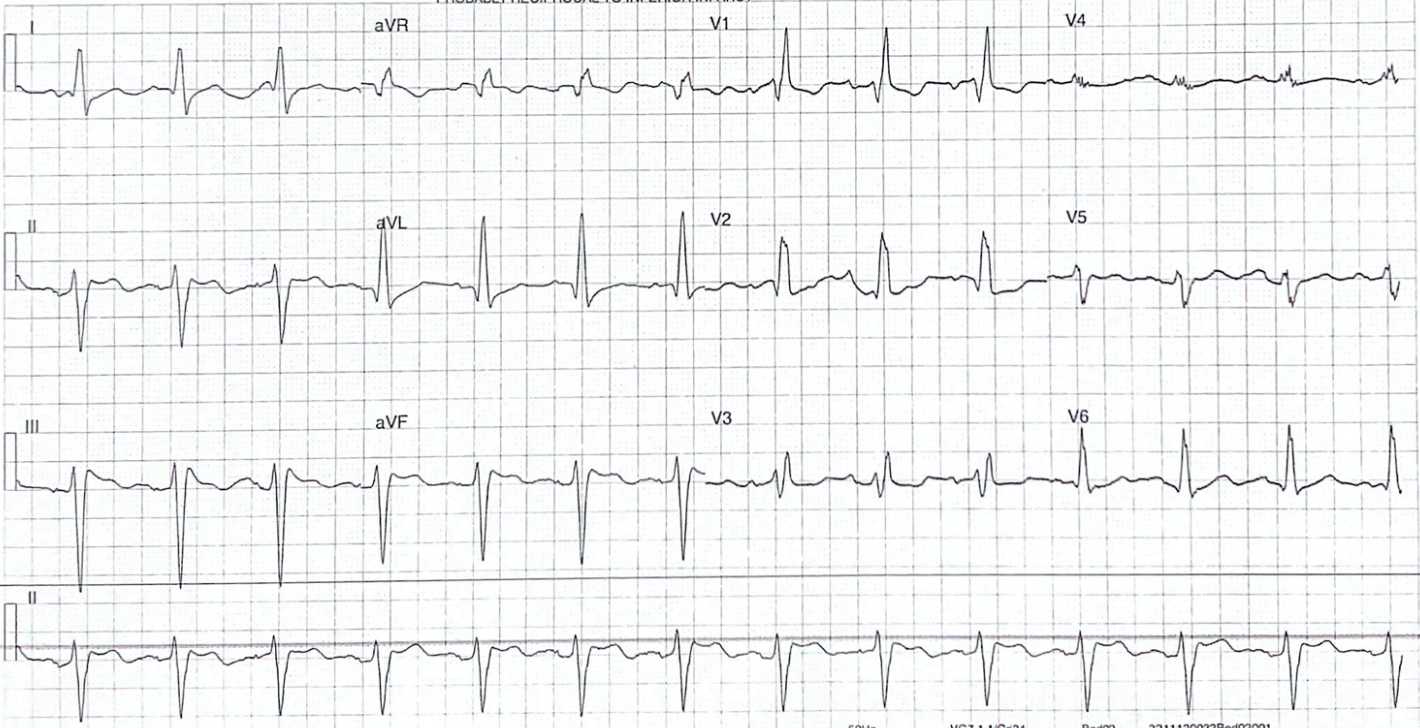
The most obvious abnormality is ST segment elevation inferiorly (II, III, aVF) in the context of RBBB morphology. Systematically, the ECG shows sinus rhythm with a rate of ~70, left axis deviation, and no AV nodal block with a normal PR interval. The QRS is wide at 160ms with right bundle branch block morphology. There is also ST segment depression in V1 – V3. The QT interval is not prolonged.
Given the patient looked well from the end of the bed, had no chest pain, was not diaphoretic or complaining of nausea, and had normal observations, the decision was made to aspirin load and await serial troponins (which returned negative). She was subsequently discharged with oral antivirals for COVID and advised to have GP follow up for further cardiac investigations and continue 100mg of Aspirin a day.