
75 years old male, brought to ED by family with increasing lethargy and generalized weakness for last few days. 2 days ago patient had a fall in shower , seen by GP same day and was advised to observe. No obvious injuries found. His past med history includes T2DM, HTN, CKD. He is visiting from INDIA and has been intermittently non compliant with his medications.
GCS 13, HR 75, BP 85 systolic , temp 35.5. Peripherally shut down.
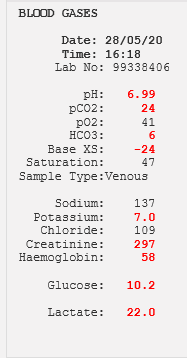
ECG : looks ischemic with STE AVR , and global STD. Following VBG is obtained:
Answer:
1: Severe metabolic acidosis.
AG= 137+7-109+6 =29.
Expected Co2= 1.5 X bicarb + 8 = 17.
Severe hyperkalemia
Severe anemia.
severe hyperlactatemia.
high creatinine
So HAGMA with partial compensation in the setting of severe anemia, kidney injury and life threatening hyperkalemia.
Differentials: Patient is clearly shocked.
C: cardiogenic shock with type A MI ( ischemic ECG)
H: Hemorrhagic shock ( low Hb) ? upper GI bleed.
O: Obstructive: no signs of tamponade or tension pneumothorax or big PE.
D: Distributive : sepsis as primary cause driving multiorgan failure . Acute on ch kidley failure with metformin contributing to high lactate and acidosis.
2: Initial resuscitation :
Airway and breathing : maintaining airway, sats 95 RA,
C: 2 wide bore IV access, 500 ml fluid bolus, Treatment of hyperkalemia with ca gluconate, insulin dextrose, salbutamol inhalers, sod bicarbonate. Activation of MTP > urgent transfusion of PRBC/ FFPs, platelets.
D: GCS 13-14. temp 35.5. no melena on PR.
E: no rash, no signs of CLD.
Further Resuscitation of this patient will be directed by further clinical information , examination, collateral from family .
Collateral from family: no previous known liver problems, no history of melena, or hematemesis, occasional ETOH drinker. no infective symptoms. no history of chest pain. Had vague mechanical thoracic area pain for which had been taking tramadol for last 2 weeks.
Medication List : antihypertensive, statin, metformin , sod bicarbonate tablets, diuretic.
PR: no melena. , Abd exam : no ascites, no signs of ch liver disease.
3: Definitive Management :
Definitive Managmenet will depend upon the underlying pathological process.
Formal Bloods : MCV 116 ( high), urea 12 ( high ). LFTs moderately deranged. CT non contrast abdomen showed cirrhotic liver changes. Patient was intubated , ventilated after initial stabilization.
Patient was admitted to ICU where he received urgent dialysis , along with ongoing blood products but remained hemodynamically unstable. Nasogastric tube drainage showed coffee ground fluid and occult UGIB was suspected , needing urgent transfer to tertiary centre for endoscopy . Endoscopy showed 3 bleeding esophageal varices.
Learning point: Low Hb in the setting of high urea and potassium in an unwell looking patient, Occult GI bleed is very likely.